Background
The gluteus medius is a hip muscle that performs hip abduction (moves hip away from the body) and stabilizes the pelvis when upright. This muscle originates on the outer surface of the ilium, inferior to the iliac crest and inserts onto the greater trochanter.
Gluteus Medius Injuries
Gluteus medius injuries often present with pain around the lateral aspect of the hip and can be classified into a bigger pain syndrome called greater trochanteric pain syndrome (GTPS) which includes several conditions that can cause lateral hip pain. The pain tends to be fairly localized to the bony prominence of the lateral hip (greater trochanter). You may have pain with lying on the affected hip at night, pain with standing for prolonged periods, pain with getting up from a chair, ascending/descending stairs, or pain/weakness moving your leg away from your body.
A gluteus medius tear may go undiagnosed for several months and can be confused for other common conditions that also localize pain to the lateral hip (i.e. trochanteric bursitis). If conservative measures fail to provide adequate results of lateral hip pain or if the history and examination suggest something different than other common conditions, advanced imaging (ultrasound or MRI) is ordered to further investigate other possible causes of pain which is when a tear is found to be present.
Injuries to the gluteus medius can result for a number of reasons. Risk factors include age (>50 yo), gender (more common in women) and obesity. Patients with gluteus medius injuries will often have a tight iliotibial band, limb-length discrepancy, back or hip structure abnormalities, overuse injuries from sports (i.e. running), trauma, or decreased blood supply to the tendon in the elderly which can lead to tendon degeneration, impaired tendon healing and eventually a tear.
Treatment
Initial treatments consist of:
If conservative therapies fail, then advanced imaging may be ordered to identify other causes of the pain. If a tear is found, this may require surgical intervention.
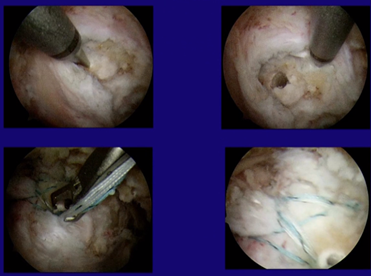
Surgery
Surgery for a gluteus medius tear can be performed in an open fashion or endoscopically. Dr. Lee prefers endoscopic repair given the excellent outcomes and decreased complication rate. This is done as an outpatient procedure.