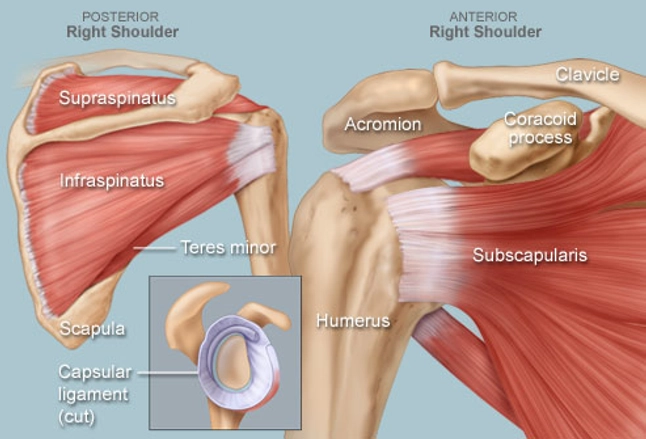
The shoulder joint is a ball and socket joint that connects the bone of the upper arm (humerus) with the shoulder blade (scapula). The shallow socket in the scapula is the glenoid cavity. The capsule is a broad ligament that surrounds and stabilizes the joint. The glenoid labrum is a rim of cartilage attached to the glenoid rim. If the arm is pulled out of its socket, the capsule and labrum tear, usually from the rim of the glenoid cavity. A dislocation occurs when the humerus comes completely out of the socket and stays out. A subluxation occurs when the humerus comes partly out of the socket and then slips back in. When the capsule tears from the glenoid rim, the shoulder can become unstable and dislocate or sublux repeatedly. The most common direction for the humeral head to dislocate is toward the front of the body (anteriorly). This typically occurs if the arm goes too far behind the body when the arm is away from the body. The humeral head can also dislocate toward the back of the body (posteriorly) when force is directed toward the back of the shoulder. This can occur when falling forward on an outstretched arm or blocking with the arm straight ahead in football.
Some patients who dislocate their shoulder do well after the injury and do not have recurrent instability. They tend to be older in age and not active in sports. Young people, especially athletes, are prone to have recurrent dislocations and subluxations and usually need surgery to correct the shoulder problem. The unstable shoulder joint can be repaired arthroscopically. In some instances, an open procedure is performed in which the muscles are separated to expose the shoulder capsule but this is rarely required. If the capsule is found to have torn away from the bone, holes are made in the glenoid rim. Stitches are passed through each hole and through the capsule and tied, securing the capsule to the glenoid rim. The capsule heals back to the bony rim and prevents the shoulder from re-dislocating. It takes several months for the capsule to heal back to the bone.
The success rate of the open Bankart repair is approximately 97%. The success rate of arthroscopic Bankart repair is similar. If there is a fracture of the glenoid rim (Bankart lesion) and a compression fracture of the humeral head (Hill-Sachs lesion), there is an increased risk of recurrent instability following repair. Procedures aimed at treating these lesions help prevent further instability.
Two nerves are at risk during surgery since they are near the operative field, but they are rarely injured. As with any surgical procedure, there are potential risks. The incidence of infection is less than 0.5%. The shoulder can lose some motion after surgery, especially if the shoulder has to be significantly tightened because of excess laxity.