Carpal Tunnel Release
Carpal Tunnel Syndrome
Carpal tunnel syndrome is the most common compressive neuropathy and accounts for roughly 90% of all compressive neuropathies. This condition is often associated with medical and mechanical risk factors. Risk factors include but are not limited to genetic predisposition, obesity, some endocrine and autoimmune disorders, pregnancy or repetitive motions.
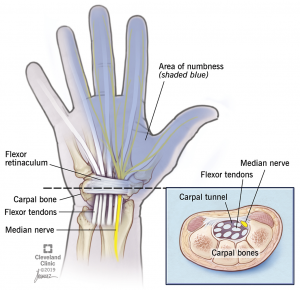
In the case of carpal tunnel, the transverse carpal ligament (also known as the flexor retinaculum) becomes thickened. This ligament sits on top of the median nerve which provides motor and sensory function to the thumb, index, middle and radial half of the ring finger. If the nerve becomes compressed by the thickened transverse carpal ligament, sensory changes such as tingling or numbness in the above fingers or motor changes such as weakening grip strength and atrophy of the thenar muscles can occur.
Treatment Options
After a thorough history and exam are conducted and carpal tunnel syndrome is thought to be the likely diagnosis, your provider will discuss further testing and treatment options for this condition. Often times, a nerve study called an electromyelogram and nerve conduction study (EMG/NCS) are ordered to ensure identification of the entrapped nerve. On occasion, a cervical (neck) impingement of a nerve can present similiar to a carpal tunnel syndrome. The EMG/NCS helps provide additional information to confirm the diagnosis.
After confirmation of the diagnosis, treatment options are discussed. These include:
- Night braces for patients with night time symptoms – Braces maintain the wrist in neutral position to avoid nerve compression.
- Anti-inflammatories
- Activity modification
- Steroid injections
- Carpal tunnel release
If a carpal tunnel released is determined to be the best option, your provider will schedule this on an outpatient basis. This is performed through a 2 cm incision on the proximal palm of the hand. The transverse carpal ligament is released and the palmar fascia and skin are then closed. A soft dressing is applied and left in place for 48 hours after which the wound should be kept clean and dry. You may re-dress the wound with a bandaid to cover the wound. The patient may shower 72 hours after surgery but no submerging the wound in water (tubs/pools/dish water/etc.) until the wound is completely healed. There is generally no formal therapy required after surgery but the below protocol is given to the patient to follow and do at home. The goal of rehabilitation after carpal tunnel release is to allow for wound healing while still maintaining the function of the fingers and wrist. Heavy gripping is prohibited for 6 weeks to allow wound healing and to prevent palmar and pillar pain (pain in the palm).
Outcomes of carpal tunnel surgery are very successful in the majority of patients, but can depend on the severity and duration of symptoms. In some patients with long standing and more severe symptoms, the goal is to stop the progression of the neuropathy but with an understanding that some symptoms may persists for several months or may even be permanent. For example, 20% of patients with severe symptoms may have residual symptoms after surgery.
See below for Dr. Lee’s postoperative recovery protocol.
Phase One – week 1-2:
You will have a soft dressing on that can be removed on postoperative day 2 and a replacement dressing can be placed
On the same day of surgery you can start moving the fingers fully. You should continue to flex and extend at least 5 times per day to prevent adhesions and wound complications
Start with the fingers full straight, then hook the fingers keeping the knuckles straight, then make a full fist. Repeat this 10 times per session.
It is okay to shower on POD 3 with no dressing on at that time
Pain is controlled with ice, ibuprofen, Tylenol (acetaminophen), and limited narcotics
Phase Two – week 3-6:
Sutures will be removed at your 2 week follow up visit
3 days after the sutures are removed, the scar needs to be massaged at a minimum of three times per day to prevent adhesions and to desensitize the region
Begin more full range of motion of the wrist and fingers
Still no heavy gripping with the operative hand but can initiate lifting
Wrist strengthening with 1-2 pound weights can be started
Begin strengthening of the abductor pollicis brevis
Phase Three – past week 6:
No restriction to function
Begin full strengthening of the hand and wrist
As with all surgery please call the clinic at 307-578-1955 if there are any concerns including abnormal redness or drainage around the wound, fevers, chills, or increasing pain.