Lateral Epicondylitis (tennis elbow)
Lateral epicondylitis, otherwise known as tennis elbow, is a painful overuse disorder involving the forearm extensor tendons as they originate from the lateral (outside) aspect of the elbow. This condition is the most common cause of elbow pain and affects men and women equally, usually in their dominant arm. Those who perform repetitive lifting/gripping activities (i.e. heavy laborers, tennis players, weight lifters, etc.) are more prone to this injury. However, this condition can be initiated by increasing one’s level of activity without proper pre-conditioning (i.e. lifting boxes when moving).
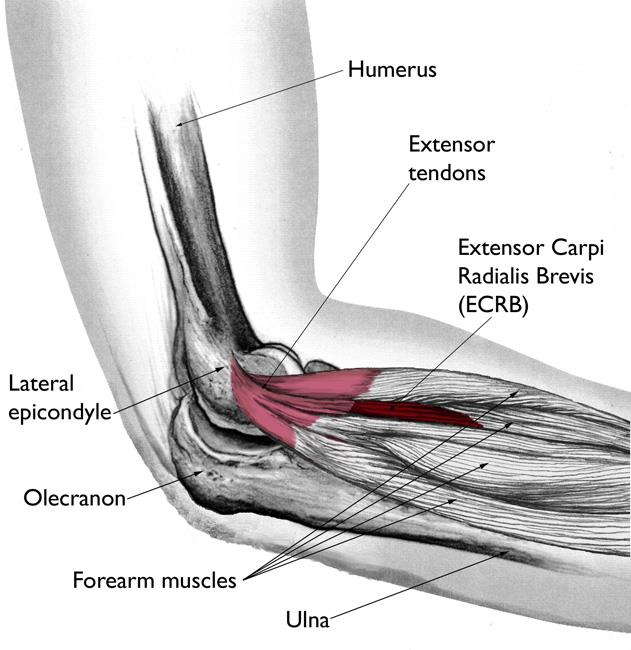
In the elbow, there are multiple tendons which come together to form the common extensor tendon. These tendons attach to the muscles in the forearm which extend to the wrist and fingers to perform wrist and finger extension when activated. When this complex of muscles and tendons undergo repetitive and/or increased activity, they can sustain micro-tears near their attachment site at the elbow (lateral epicondyle). Given the fact that we as people continuously use our hands and lift objects, a cycle of healing and re-injury can occur, thus prolonging the ability to heal this injury. In addition to repetitive injury, the tendons generally have a poor blood supply which can further complicate the healing process. As a result, this injury can be quite nagging unless appropriately treated.
carpi radialis brevis.
Signs and symptoms of tennis elbow involve pain over the lateral elbow which is often aggravated with resisted wrist and finger extension or gripping activities. Sometimes, the patient may have decreased grip strength. There will also be point tenderness over the common extensor tendon.
Initial treatment options for tennis elbow include avoidance of aggravating factors, NSAIDs, ice, and physical/occupational therapy. Tennis elbow straps and wrist braces at night (to prevent wrist extension) are also treatment options. Often times, a steroid injection is provided to provide quicker relief. It is estimated that this condition resolves in roughly 95% of patients but may take several months before relief is obtained.
If conservative therapy fails, then a discussion for surgical intervention may be had. Dr. Lee performs an open release of the ECRB tendon with debridement of the damaged tissue. The tendon is subsequently repaired and the patient is placed into a long arm splint to allow the wound to heal and to protect the repair. The splint is removed at the two week postop visit and the patient is transitioned to a wrist brace to prevent wrist extension and tension on the repair. Gentle elbow range of motion may begin at this time. No gripping is permitted for 6 wks. At 6 wks postop gentle strengthening may begin. Usually by 3 months after surgery, the patient is returned to full activity.